

There is a good deal of controversy regarding how Christians and abolitionists more specifically should think about ectopic pregnancy treatments. This article will give an overview of what ectopic pregnancy is, how the current medical field treats it, and how the current medical field SHOULD treat it.
What is an Ectopic Pregnancy?
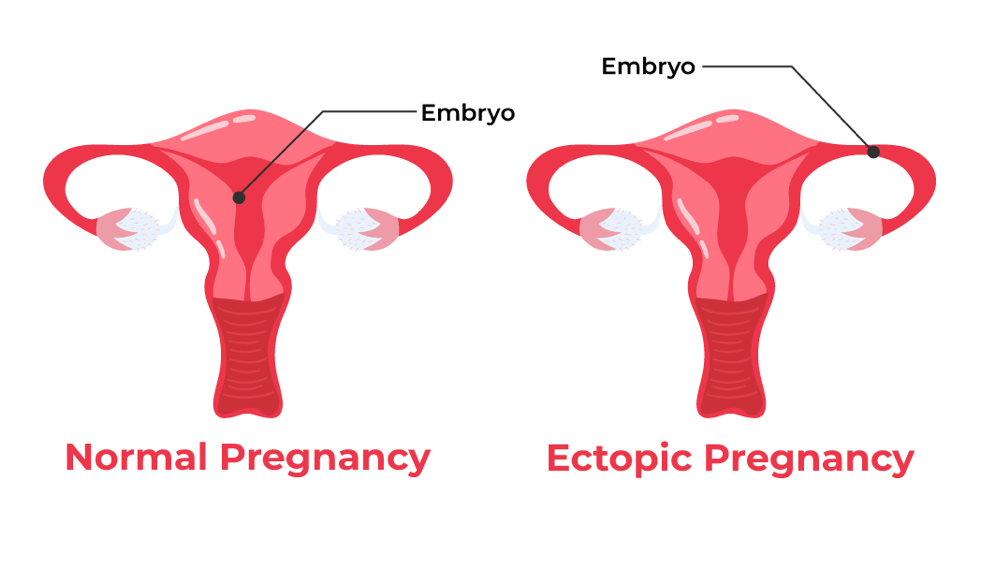
An ectopic pregnancy, also referred to as an extrauterine pregnancy, is a pregnancy in which the baby has implanted in an abnormal location outside of the uterus. In most ectopic pregnancies, the baby is inside the fallopian tube. This is called a tubal pregnancy. In tubal ectopic pregnancies, the mother presents symptoms of pelvic pain, spotting, nausea, and abnormal hCG levels.
Tubal ectopic pregnancies are often diagnosed before 7 weeks LMP, (dated from last menstrual period). By this time, the baby has usually already died, as the fallopian tubes are not equipped to sustain a growing baby. The danger with a tubal pregnancy is that fallopian tubes have lots of blood vessels (meaning lots of potential for bleeding if ruptured) and are not very elastic (meaning it cannot appropriately expand as the baby grows). If it ruptures, the mother will suffer internal bleeding which can cause maternal death if immediate treatment is not administered, usually involving surgery to remove the fallopian tube, as detailed later.
Tubal pregnancies are 90% of ectopic pregnancies, but 10% of the time, the baby implants elsewhere in the abdominal cavity (such as on the cervix, ovary, myometrium, interstitial portion of the fallopian tube, abdominal cavity wall, or within a cesarean section scar). These babies have a better chance of survival, especially if the mother has endometriosis which means an abnormal placement of endometrial tissue outside the uterus. There are many reported cases of babies surviving non-tubal ectopic pregnancies. (See links at the bottom for examples.)
Using technologies including ultrasounds, doctors can detect where in the abdomen the baby has implanted and whether the baby is still alive. Whether or not the baby is still alive, we will be able to see chorionic villi (the primitive cells that would make the placenta), maternal blood, pregnancy cells and debris, and a microscopic baby.
Current Medical Practice
As we address in the following paragraphs the current medical practices contrasted with what we believe are morally acceptable treatment practices, be sure to understand clearly our distinction between the case of a living child in an ectopic pregnancy, and the case of an already deceased child in an ectopic pregnancy.
Whether or not the baby is found alive, the current approach for medical professionals is often to immediately intervene to remove the baby. This intervention can take the form of surgery to remove the baby from the fallopian tube or to remove all or part of the fallopian tube, (salpingostomy, salpingectomy, or partial salpingectomy). It can also take the form of a drug called Methotrexate used to chemically stop pregnancy growth and kill the baby if the baby is still alive. Even if the baby is not living, other pregnancy cells, such as the chorionic villi and amnion, can be, and this cell growth needs to be halted, in some cases immediately. Chemical treatment is not as effective as surgery, but it is less invasive, and some doctors give it a try at first to see if it will dissolve the area of concern. Methotrexate can only be used if the baby is very small, and the mother is stable.
None of these surgical and chemical interventions, if performed when the baby has already died, is an abortion. It is always ethically permissible and often medically necessary to use medical intervention to remove a deceased baby from the mother. In many cases, however, no medical intervention is necessary, so doctors sometimes do not pursue either surgical or chemical intervention, but instead practice watchful waiting, also referred to medically as expectant management. Research has shown that, in patients with an ectopic pregnancy who are properly assessed and their hCG levels are dropping, roughly 50% will end and be passed naturally with no need for surgical or chemical intervention.
Our Position
Most babies have already died by the time the ectopic pregnancy is diagnosed. However, when the baby is still alive, we do not believe the above surgical and chemical interventions, which cause the death of the baby, are morally permissible. The ethical treatment in these cases is watchful waiting/expectant management and an attempted transplant of the baby to the uterus if the mother’s condition worsens.
If the doctor and patient choose to pursue expectant management and the mother is stable, she can be sent home with very strict instructions about what to watch for and what to do if things start going downhill. If she is already in an unstable condition, she should be admitted to the hospital immediately. In either case, doctors should monitor her vital signs, hCG levels, and perform regular ultrasounds.
All of the current surgical and chemical intervention options, performed while the baby is still alive, result in the death of a living baby. We believe that such actions are premature and unethical. On top of being premature, we believe that this response, even though it may not be the intent, is a sort of shrugging off the value of the life in the womb, proverbially throwing one’s hands in the air as to anything that could be done to attempt to save the baby. The oath medical professionals take to “do no harm” and their duty to attempt to save every life should require them to recognize they have a second patient in the womb and at least try to save the life of the baby through a procedure that involves surgically removing the baby from the fallopian tube and placing the baby in the uterus with the hope that he or she will reattach. Most medical professionals do not believe that successfully reimplanting the baby in the uterus is possible, but there are some who do, including a hospital in China that reports an embryo reimplantation success rate comparable to IVF!
Imagine the current medical field’s response to a situation like ectopic pregnancy, but instead of a preborn child and a mother, it was happening with a newborn child and a mother. In the thought experiment, doctors do not believe it is likely or possible that a newborn can be saved with ____ condition, a condition that also somehow threatens the mother’s life. So instead of taking any (even long shot) action attempting to save both or expanding research efforts to find ways to save the newborn child, they immediately take a course of action that they know will directly result in the newborn’s death. They would likely lose their license to practice medicine if they intentionally killed the newborn without lifting a finger to try to save him. Depending on the exact situation, they could even face criminal charges. But because our culture and laws do not recognize the life in the womb as equal in value to born humans, the medical community has disregarded ectopic life and shown a lack of interest in continuing research on saving ectopic babies. The current medical response is irresponsible and negligent to their oaths and duty to equally treat every human being as a patient with intrinsic value.
Ultimately, our position is that the ethical treatment of an ectopic pregnancy in the case of a baby who is still alive involves watchful waiting/expectant management or an attempted transplant of the baby into the uterus. If, during watchful waiting/expectant management, the mother’s condition worsens and there are signs of a fallopian tube about to rupture or some other medical emergency while the baby is still living, a transplant should be immediately attempted.
Important note: some ovarian cysts mimic early ectopic pregnancies. When a woman is stable under watchful waiting, sometimes, what was first thought to be an ectopic pregnancy turns out to be just a corpus luteal cyst and the fact that she has a normal intrauterine pregnancy (IUP) is then later seen. For this reason, some medical professionals advise against the use of chemical intervention of Methotrexate due to risks and misdiagnosis of both mother and baby. Misdiagnosis of an ectopic pregnancy and subsequent treatment could lead to the completely unnecessary death of a healthy baby in a normal, intrauterine pregnancy and sometimes complications for the mother.
Another note: when someone at a surgical abortion facility tells you that they are there to have an ectopic pregnancy treated, they are lying. Ectopic pregnancies are real medical conditions that need to be monitored and treated through a hospital. They cannot be treated at an abortion facility. Surgical abortion facilities are designed to dilate and scrape the inside of the uterus only going through the vaginal vault and cervix. There are no abdominal incisions. No surgery on tubes. These facilities are not set up like that because they are not in the business of true medical care. That is not their purpose. And although they can dispense pills for an intrauterine (normal) pregnancy, they cannot dispense pills for an extrauterine pregnancy. Abortion pills to contract the uterus are different from pills to treat an ectopic condition. Also, ectopic pregnancy situations are true medical emergencies that require prompt attention, she needs to go to the ER, not make an appointment for next Wednesday at Planned Parenthood.
Links for further research:
Innovative Ectopic Pregnancy Intrauterine Transfer Surgery: Granting a Lifeline for Life
Could This Lead to Saving Ectopic Babies?
Miracle baby was carried outside mother’s womb
I carried ectopic pregnancy for nine months without knowing
Baby is born alive after growing in mother’s abdomen for 29 weeks
The mother who risked everything to have her ectopic baby
Baby born after rare ectopic pregnancy
Surviving Fetus from a Full-Term Abdominal Pregnancy
Ectopic triplet makes medical history
Transplantations of Ectopic Pregnancy from Fallopian Tube to Cavity of Uterus
Term Spontaneous Heterotopic Pregnancy (Abdominal and Intrauterine): A Case Report


